
What am I looking at?
The trustees of Scottish cancer charity Let’s Talk About Mouth Cancer give an overview of the signs, symptoms and best practice when it comes to diagnosing a potential mouth cancer
We are all too aware that mouth cancer is on the rise. More and more cases are being diagnosed every year with about 300,000 cases of lip and oral cancer reported globally1. In 2014, there were 7,680 cases of oral cancer in the UK2 and, since 1970 there has been a 93 per cent increase in the number of cases3.
Scotland remains a hot spot for oral cancer with higher incidence rates and lifetime risk compared to the rest of the UK.
Cancer Research UK predicts a further 33 per cent increase in oral cancer by 20353. Clearly, we need to act now to address this increasing problem. We, as a profession, have it within our power to do something; stand up, speak out and make some noise about mouth cancer. Our training and position in the community make us the ideal group of health care professionals to provide counsel to patients on risk reduction, screen for the disease and to empower patients with skills and knowledge to find the disease themselves at an early stage.
Risk factors
Traditionally, this has been a disease that affected older men. They have often smoked tobacco and drunk alcohol for many years. Now, that picture is beginning to change. Smoking and alcohol still remain important risk factors but more young people and women are developing this disease without traditional risk factors. Nine out of 10 cases of mouth cancer can be linked to a preventable cause4. Other risk factors include a diet low in fruit and vegetables, poor oral hygiene and the Human Papilloma Virus infection.
With global migration increasing it is likely we will see an increase in the use of smokeless tobacco, areca nut and betel quid in Scotland. There is also growing evidence of the adverse effect that shisha smoking has on health5. Therefore, we must think beyond the traditional risk factors.
A recent study revealed that the vast majority of patients developing head and neck cancer in Scotland are from the most deprived areas in our communities, therefore suggesting that this is a disease of inequality6. In fact, the deprivation gap for mouth cancer is the third highest amongst all cancers at 117 per cent7. Public health initiatives should take this into account when developing measures to address the burden of mouth cancer.
Prognosis
Dentists need to be vigilant when examining and screening our patients; we should have clear protocols and pathways in place for managing suspicious lesions and reviewing those lesions or mouths that simply ‘don’t look right’. Early detection is still recognised as the most important prognostic factor in mouth cancer8. Other prognostic factors include the aggressive nature of the tumour and the proliferation rate of the cells9.
Currently, the mainstay treatment for mouth cancer is high morbidity surgery. As a result of such major surgery, patients’ quality of life post surgery is vastly reduced. Treatment impacts on all aspects of life that we take for granted, such as enjoying meals, conversing freely and showing affection to loved ones. Although there have been great advances using free flap tissue repair to reconstruct surgical excision sites, this has had little to no impact on survival and prognosis, with only 53 per cent of patients surviving to five years post diagnosis10. Those that receive an early diagnosis have an 80-90 per cent chance of survival at five years. While those that present late with advanced disease have a much lower survival or if there is spread to other body systems then treatment is likely to be palliative.
Mouth cancer referral guidance
Dental patients should be examined for signs of malignancy as a part of the routine oral examination at every visit. The Scottish Referral Guidelines for suspected oral cancer11 identify a number of signs and symptoms which may represent malignancy (see Table 1 below). The guidelines recommend that those patients who present with the identified signs and symptoms which last for more than three weeks should be referred urgently to a specialist service according to local referral protocols.
The National Institute for Health and Care Excellence12 (NICE NG12) make similar recommendations and advise that patients who are referred urgently with suspected cancer should be given an appointment in the specialist service within two weeks of referral.
To improve early detection and thus survival, Scottish-based charity Let’s Talk About Mouth Cancer (LTAMC) work directly with the public as well as with professional groups. We advocate a shorter timescale than three weeks, instead recommending that patients should be referred urgently when signs and/or symptoms which are suspicious of mouth cancer do not resolve after just two weeks. The aim of this initiative is to reduce diagnostic delay as much as possible.

Diagnostic delay
Patient delay and professional delay contribute to the total diagnostic delay.
Patient delay
This is defined as “the period between the patient first noticing symptoms and their first consultation with a health care professional concerning those symptoms”13.
Approximately 30 per cent of patients diagnosed with mouth cancer will wait three months following the self discovery of signs and symptoms before attending a doctor or dentist14, 15. This may be because they attribute the symptoms to non-malignant, self-correcting conditions.
A study by Scott et al (2008)13 found that patients with better knowledge of signs and symptoms of mouth cancer are less likely to delay seeking advice. Knowledge about mouth cancer aids interpretation of symptoms and the decision to seek help. The same study also found that a low socio-economic background and deprivation are significantly higher in patients who delay seeking help. These patients also experience real or perceived limited ability to access healthcare. Some of the work of LTAMC aims to rectify some of these issues by educating the public about the signs and symptoms of mouth cancer, focusing on deprived and minority community groups.
Professional delay
It has been shown that lack of knowledge by general dental and medical practitioners about the signs, symptoms and risk factors of mouth cancer can also contribute to the delay in diagnosis. Patients will frequently present first to their doctor with mouth symptoms. A cross-sectional study in Dundee found that, compared to dentists, a significant number of doctors felt they had insufficient knowledge about the detection and prevention of mouth cancer16. Waiting lists and pressures in the health service may also contribute further to professional delay.
How to spot mouth cancer
As recommended in the guidelines, every patient attending for routine check-up should have a full head and neck soft tissue examination. A systematic approach should be routinely used to avoid missing any areas. A video of this can be seen on our website (www.ltamc.org/professional-resources).
Before any examination, a detailed history should be taken. For each area of concern, the patient should be asked about the length of time they have been aware of the lesion/symptoms and ascertain if there has been any pain, change in sensation or effect on function (speech, swallowing, eating). In many cases, however, early and even late tumours can be asymptomatic. It is also worth asking if a lesion has been present before and healed fully or partially. Of course, if the patient is unaware of the area, then questioning may be delayed until after detecting a suspicious lesion.
Extra-orally, the soft tissues should be checked for any asymmetry, swellings or lymphadenopathy; it is important to note any changes in texture and fixation. A hard, fixed lump in the neck is highly suggestive of tumour spread to the lymph nodes.
Intra-orally the oral mucosa has natural variation according to its anatomical site. It is important to be familiar with normal appearances as any changes need to be investigated. The Scottish Cancer Referral Guidelines11 recommend referral for cancer arising from the oral mucosa when there are persistent unexplained lumps, ulceration, unexplained swellings, red or mixed red and white patches of the oral mucosa. Proper and clear description of any lesion is fundamental, both for the sake of good record keeping and also to allow any referral to be as fulsome and informative as possible.
To cover all aspects of a lesion, these characteristics should be recorded and described:
- Site – where the lesion is, note adjacent structures
- Size – can be measured in millimetres with probe/ruler or relative to local anatomy (e.g. extending from mesial 34 to distal 36)
- Colour – red, white or mixed (homogeneous/heterogeneous)
- Texture – hard or soft, fixed or mobile, smooth or rough, induration
- Border – well or poorly defined, raised or flat.
Based on all these findings, a decision must be made whether to monitor in practice, make a routine referral or to refer urgently. It is not necessary to arrive at a definitive diagnosis, rather a decision to refer for further investigation and appropriate treatment. The patient should be informed of the findings, possible diagnosis and also the reasoning for referral or monitoring in practice. The importance of attending arranged appointments must be stressed.

Click to open full size
Referrals quiz
Let’s take a few examples and put this into practice. Look at each of the cases below and their brief history. Try describing each as you would for a referral and decide whether you would monitor in practice, make a routine referral or refer urgently. Have a guess at the diagnosis as well. Remember, the triaging surgeon ultimately decides from your referral whether to allocate as urgent or routine, so quality of information is key.
Many lesions are not clear cut and easy to decide on management. You are not alone – if in doubt, seek the opinion of a colleague or send in a referral. In this case, the description and history you submit is essential for the receiving surgeon to adequately assess the urgency for appointment. Be reassured that the majority of urgent referrals after investigation are not cancerous but it is only possible to know that after appropriate tests.
It is vital to follow up a patient where the decision to monitor a lesion within practice or a routine referral has been made. In the instance there are any changes to the area, reconsider if the original decision needs to be altered. Likewise, when managing a lesion in practice first (e.g. ease traumatic denture, smooth sharp edge on tooth, prescribe antifungals), this must be reviewed after two weeks to gauge response. If not healed, then reappraise the suspected cause, treatment provided and potentially send a referral. Also, if the patient misses an appointment or has not received one within the expected time frame, contact the department to ensure one is arranged.
-

- Case one – Patient: Female, 34, with no symptoms, all feels soft. Clinical description: Stellate reticular white lesion, right buccal mucosa, adjacent to amalgam restoration.

-

- Case two – Patient: Male, 61, no pain, present for more than three weeks. Smoker. Soft on palpation. Clinical description: Well defined but non-homogenous mixed white and red lesion on dorsum of tongue.

-

- Case three – Patient: Female, 59, no pain but changed speech for one month. Clinical description: Right lateral tongue raised rolled margins with necrotic centre, firm and fixed on palpation. Hard fixed lumps felt in right neck.
-

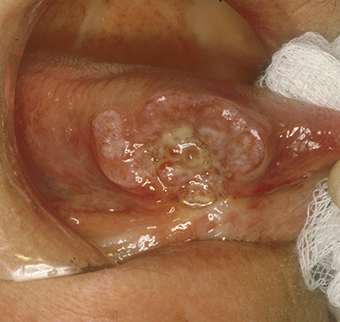
- Case four – Patient: Male, 45, of Asian origin, painful large sore areas for more than three weeks, history of tobacco chewing. Clinical description: Large area of exophytic-type (cauliflower-like growths) affecting maxillary alveolus.

-

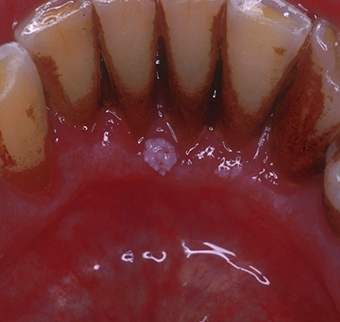
- Case five – Patient: Male, 46, non-painful lesion for one to two weeks. Clinical description: Asymptomatic gingival 3mm in diameter, sessile papillomatous-like lesion.
-

- Case six – Patient: Female, 55, painful mouth for more than three weeks. Clinical description: Well defined 2cm lesion on floor of mouth with raised rolled margins with necrotic centre, firm and fixed on palpation. Associated left neck swelling.

(Quiz answers are at the end of the article)
Empowering our patients
Recently, LTAMC has developed its strategy away from clinician-based screening in favour of patient empowerment – the focus has changed to teaching self examination for mouth cancer. Although a conventional oral examination by a clinician remains the most sensitive and specific method to detect mouth cancer cases17, teaching mouth cancer self examination empowers patients to recognise pathology in their mouth and may increase awareness.
A Cochrane review published in 2013 found that mouth cancer self examination had similar sensitivity and specificity to breast self examination17. Teaching mouth cancer self examination can be used as a tool in general practice to increase awareness of mouth cancer. It can form part of a general discussion about the signs, symptoms and risk factors of mouth cancer. The thorough, logical mouth self examination process follows five simple steps and is demonstrated in the graphic above. The key messages are to check for: red or white patches; lumps in the mouth that grow; ulcers in the mouth that do not heal; and persistent soreness/discomfort.
The advice is to attend the dentist or general medical practitioner if any of these signs/symptoms do not resolve in two weeks and importantly, to alert the practitioner to a concern about mouth cancer. Patients should be encouraged that mouth self examination is easy, and only requires a light source and a mirror. The aim is simply to empower patients to recognise normal tissues, and to present early if something changes. The mantra “If in doubt, check it out” should be repeated often.
LTAMC has also produced an instructive video aimed at teaching the general public how to perform a mouth cancer self examination. It can be found at youtu.be/WQaujHXauso
The video has been viewed more than 4,500 times in the UK, USA, Japan, Vietnam and India, indicating a worldwide interest. As mentioned above, a recent study has shown that approximately 30 per cent of patients with mouth cancer delay seeking help following discovery of symptoms for more than three months13. As early diagnosis is a key factor for improving prognosis and survival, we as dentists must tackle the lack of recognition of symptoms among our patients.
Lack of insight into initial symptom interpretation and lack of knowledge of mouth cancer have been shown to be significant variables which contribute to patient delay in seeking help13, and are issues that may be easily modified with targeted interventions by general dental practitioners.
Conclusions
Mouth cancer is increasing at an alarming rate and yet large sections of the public know little of the risk factors or signs and symptoms of the disease. Despite the fact that about half the population attend a dentist regularly for dental check-ups, many cases present at a late stage with a correspondingly poor prognosis. Survival has not improved substantially in the past 50 years and there is no treatment available that can transform the poor survival of someone with late stage disease to the much better survival of someone with early stage disease; the only thing that can do this is early diagnosis.
The work of LTAMC is firmly focused on teaching the public as well as professionals to diagnose mouth cancer early. We hope to break down health inequalities and empower as many people as possible to recognise the disease and its risk factors to improve survival. We call it our empowerment journey, so “Let’s talk about mouth cancer!”
Quiz Answers:
Case one
Outcome: Monitor in practice.
Diagnosis: Lichenoid lesion/lichen planus.
Case two
Outcome: Urgent referral.
Diagnosis: Dysplastic lesion or early cancer.
Case three
Outcome: Urgent referral.
Diagnosis: Squamous cell carcinoma.
Case four
Outcome: Urgent referral.
Diagnosis: Squamous cell carcinoma.
Case five
Outcome: Routine referral.
Diagnosis: Human Papillomavirus related papilloma.
Case six
Outcome: Urgent referral.
Diagnosis: Squamous cell carcinoma.
About the authors
This article was co-authored by the five trustees of the Scottish charity Let’s talk about mouth cancer (SC045100):
- Dr Niall McGoldrick BDS MFDS RCPS(Glasg), specialty registrar in dental public health.
- Mr Ewan MacKessack-Leitch BDS(Hons) MFDS RCPS(Glasg), GDP, Fife.
- Dr Stephanie Sammut FDS (OS), MClinDent, MOral Surg, MFDSRCPS,
consultant oral surgeon. - Dr Orna Ni Choileain BDS(Hons) MFDS RCSEd, medical student,
Trinity College Dublin. - Prof Victor Lopes PhD FRCS, consultant maxillofacial surgeon.
Website: www.ltamc.org
Twitter: @couldbeUrmouth
Facebook: www.facebook.com/letstalkaboutmouthcancer
References
1. N Johnson, A Chaturvedi: Global burden of oral cavity and pharyngeal cancers, Global Oral Cancer Forum: 2016
2. C R Smittenaar, K A Petersen, K Stewart, N Moitt. Cancer incidence and mortality projections in the UK until 2035. Br J Cancer. 2016 Oct 25; 115(9): 1147–1155
3. www.cancerresearchuk.org [Internet]. 2017 Available from:
www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/oral-cancer#heading-Zero
4. www.cancerresearchuk.org [Internet]. 2017 Available from:
www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/head-and-neck-cancers/risk-factors#heading-Zero
5. Ziad M El-Zaatari, Hassan A Chami, Ghazi S Zaatari Health effects associated with waterpipe smoking. Tob Control. 2015 Mar; 24(Suppl 1): i31–i43.
6. Purkayastha M, McMahon AD2, Gibson J, Conway DI. Trends of oral cavity, oropharyngeal and laryngeal cancer incidence in Scotland (1975-2012) – A socioeconomic perspective. Oral Oncol. 2016 Oct; 70-5. doi: 10.1016/j.oraloncology.2016.08.015. Epub 2016 Aug 31.
7. www.cancerresearchuk.org [Internet]. 2017 Available from
www.cancerresearchuk.org/health-professional/cancer-statistics/incidence/deprivation-gradient#heading-One
8. Gómez, I., Seoane, J., Varela-Centelles, P., Diz, P. and Takkouche, B. (2009), Is diagnostic delay related to advanced-stage oral cancer? A meta-analysis. European Journal of Oral Sciences, 117: 541–546. doi:10.1111/j.1600-0722.2009.00672.x
9. Warnakulasuriya S. Prognostic and predictive markers for oral squamous cell carcinoma: The importance of clinical, pathological and molecular markers. Saudi J Med Med Sci 2014;2:12-6
10: www.cancerresearchuk.org [Internet ]Available from
www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/head-and-neck-cancers/survival#heading-Zero
11. Healthcare improvement Scotland. Scottish referral guidelines for suspected cancer 2013 ( updated in August 2014) available online
www.healthcareimprovementscotland.org/our_work/cancer_care_improvement/programme_resources/scottish_referral_guidelines.aspx [last accessed 31 July 2017]
12. National Institute for health care and excellence. Suspected cancer: recognition and referral – NICE Guideline NG12. 2015 (last updated July 2017) available online www.nice.org.uk/guidance/ng12/resources/suspected-cancer-recognition-and-referral-pdf-1837268071621 [last accessed 31 July 2017]
13. Scott S, McGurk M, Grunfeld E. Patient delay for potentially malignant oral symptoms. Eur J Oral Sci. 2008;116 2:141–147.
14. Scott SE, Grunfeld EA, McGurk M. Patient’s delay in oral cancer: a systematic review. Community Dent Oral Epidemiol. 2006;34 5:337–343.
15. Allison P, Locker D, Feine JS. The role of diagnostic delays in the prognosis of oral cancer: a review of the literature. Oral Oncol. 1998;34 3:161–170. [PubMed]
16. Carter L, Ogden GR Oral Cancer awareness of general medical and general dental practitioners Br Dent J. 2007 Sep 8;203(5):E10; discussion 248-9. Epub 2007 13 Jul.
17. Walsh T, Liu JLY, Brocklehurst P, Glenny AM, Lingen M, Kerr AR, Ogden G, Warnakulasuriya S, Scully C. Clinical assessment to screen for the detection of oral cavity cancer and potentially malignant disorders in apparently healthy adults. Cochrane Database of Systematic Reviews 2013, Issue 11.
CPD responses closed
The CPD quiz for this article is now closed. Please check the listings for the current quizzeslistings
Comments are closed here.