
Prefabricated crowns for primary molars
How to achieve full coronal coverage in primary molar restorations

In children, the goal is to restore the tooth once for the lifetime of that tooth, yet full coverage restorations for primary teeth are underutilised in general practice.
The function of a crown is to protect existing tooth structure and to retain the tooth in function. Numerous clinical situations require full coverage restorations in primary molars in order to provide the most durable restoration (Table 1). Primary teeth with extensive caries can be restored most successfully with crowns. Enamel hypoplasia of the primary molars may require replacement of cusp anatomy which is also best achieved by full
coverage restoration.
Crowns also provide an optimal coronal seal for pulpally treated primary molars; research shows that indirect pulp therapy, pulpotomy and pulpectomy procedures have better outcomes as clinical success depends on protecting the tooth from the oral environment. Protection of the dentinal-pulpal complex from contamination of the oral environment also promotes healing and protects the vitality of reversibly inflamed pulp, eliminating the need for pulp therapy.
Crowns are also indicated for developmental defects of the tooth structure; teeth with extensive tooth surface loss due to attrition, abrasion, or erosion; fractured primary molars; and infra-occluded primary molars to maintain mesio-distal space (Seale and Randall 2015).
Classification of prefabricated crowns for primary molars
All prefabricated crowns for primary molars are available in varying sizes for each primary tooth type. The manufacturers seeks to replicate the height, mesio-distal width, contour and anatomy of the natural primary teeth, specifically to accommodate the convexity of the cervical margins and the exaggerated mesio-buccal bulge on primary first molars.
Stainless steel crowns (SSCs) or preformed metal crowns (PMCs) are widely recognised for their strength and longevity; however, due to the metallic colour, they lack aesthetics (Fig 1) (Seale and Randall 2015). Chair-side techniques for direct veneering and open-facing have been used to mask the metal colour. Over the years, alternative tooth coloured full coverage restorations have been tested using different types of dental materials and techniques with varied levels of success. Commercially fabricated preveneered SSCs combine durability and aesthetics (Leith and O’Connell, 2011; Kratunova and O’Connell, 2014; O’Connell et al. 2013). Prefabricated crowns made from composite resin, high density polymers, polycarbonate and zirconia offer a tooth coloured alternatives (Fig 2).
| INDICATIONS FOR FULL COVERAGE RESTORATIONS |
|---|
| Extensive tooth destruction – caries, erosion, developmental defects |
| Caries with > two surface involvement |
| Post pulp therapy |
| Fractured molars |
| Infra-occluding molars: to maintain mesio-distal space |
| Patients with high caries susceptibility/OH impairment /special needs |
| Caries lesions restored under general anaesthesia |
Conventional stainless steel crowns
Stainless steel crowns (SSCs) are prefabricated extra-coronal restorations which can be adapted to individual teeth and cemented in place to provide a definitive restoration (Kindelan et. al. 2008). The SSC is a durable, cost effective, minimally technique sensitive restorative option that offers the advantage of full coverage and accommodates the majority of treatment indications for primary posterior teeth (Seale and Randall 2015).
SSCs were popularised as a restorative method for primary molars in the 1950s (Humphrey 1950; Engel 1950). Over time, SSCs have been modified to improve the anatomical form and the alloy composition (9-12 per cent nickel; chromium 12-30 percent) (Randall 2002). The conventional SSCs are pre-trimmed, pre-contoured and crimped and usually need no or minimal adjustment by the operator. The conventional tooth preparation requires local anaesthesia and the tooth is prepared with 1-1.5mm occlusal reduction and minimal proximal reduction of the primary molar to allow for the crown thickness (0.2mm). The armamentarium required for placement of a SSC is outlined in Table 2.
| TABLE 2 | ||
|---|---|---|
| Armamentarium required for placement of conventional stainless steel |
||
| BURS | Occlusal reduction - Football Proximal reduction - Flame |  |
| SSC INSTRUMENTS | Crimping Pliers Gordon Contouring Pliers Johnsons contouring Pliers Howe Pliers Bee Bee Curved Crown scissors Band seater |  |
| SSC KITS | Available from the major manufacturers either retrimmed, crimped and contoured, or pretrimmed with paralled walls |  |
The finish line should be a smooth feather edge at or below the gingival margin with no step or shoulder. A snap fit is achieved when the flexible metal margin passes over the buccal bulbous area and fits into the cervical constriction of the molar. SSC margins can be well adapted into the undercut areas with the help of contouring and crimping pliers (Randall 2002). SSCs cannot be used in children with nickel sensitivity. Any self-curing luting cement can be used to secure these crowns, with glass ionomer being the most popular material.
Stainless steel crowns using Hall technique
There is growing evidence that a biological approach to management of caries is effective (Kidd 2004; Ricketts et al. 2006; Thompson et al. 2008) and the technique is now gaining popularity worldwide. Isolating the caries in the tooth using a crown (sealing in caries) isolates the microflora from their nutrients reducing/eliminating their ability to cause demineralisation. The dentinal-pulpal complex is also protected from the oral environment arresting the caries process, and maintaining of the vitality of reversibly inflamed pulp.
Placement of a SSC on carious primary molars without any prior tooth preparation, decay removal, or local anaesthesia is known as the ‘Hall Technique’, named after Dr Norna Hall who had used this novel method in her clinical practice since the 1980s. The indications for Hall crowns are the same as those of conventional SSCs but cannot be used where there is a diagnosis of irreversible pulpitis or dental sepsis (Innes et al. 2009, 2011).
Success of the Hall technique relies on correct pulpal diagnosis. There is no need for local anaesthesia as there is no reduction of tooth structure and no caries is removed. The crown is filled with a glass ionomer cement and pushed onto the tooth thereby sealing the caries lesion from the oral environment. Sometimes, it is necessary to use orthodontic separators and a band seater to allow easier seating (Fig 3). Evidence of the clinical success of this technique after five years is very promising (Innes et al. 2011).
The crown is cemented onto an unprepared tooth causing a premature contact on that tooth. This increase in the vertical dimension of occlusion seems to be of little consequence in children, as occlusal equilibrium is re-established within two to four weeks, without any symptoms (Gallagher et al. 2014).
Preveneered stainless steel crowns
The increasing demand for a more natural appearance of primary tooth restorations led to the introduction of the commercially produced aesthetic preveneered stainless steel crowns (VSSCs) for paediatric dental patients. Recent developments in dental materials result in thermoplastic, composite or epoxy resin veneers to be bonded successfully to base metal using mechanical retention and/or chemical bonding (Hosoya et al. 2002).
The VSSCs were developed to combine the strength and durability of the conventional SSCs with the aesthetically pleasing appearance of the white veneer facing (Figure 4a, 4b). The exact specifications of the attachment, thickness and pattern of the veneer remains proprietary to the individual manufacturer. However, the makers of the current leading brands VSSCs (Nusmile, www.nusmilecrowns.com – and Kinderkrowns – www.kinderkrowns.com) have disclosed that the veneer is a composite resin material which is attached either through an intermediate bonding agent to the pre-prepared (e.g. alumina blasted) metal surface or is bonded and additionally mechanically retained to a fenestrated stainless steel core in different patterns (Fig 5).
The composite facing material requires adequate thickness for mechanical strength and ability to withstand occlusal masticatory forces. Therefore, the tooth preparation for a VSSC has to be modified to allow for this increased bulk in the occlusal and buccal surface. Greater buccal reduction is required. Local anaesthesia is required for tooth preparation with 1.5mm occlusal reduction.
Circumferential reduction is required to remove any cervical undercuts as the crown must fit passively onto the tooth. The finish line is 1mm below the gingival margin. This reduction of tooth structure is much greater than conventional SSC crown preparation but does not result in exposure of the pulp. Pulp therapy will be dictated by the extent of caries. VSSCs cannot be crimped in the areas of the facing so that limited crimping is advised only on the metal margins.
Manufacturers also warn that the metal substructure flexes from pressure during crimping, fitting or seating and this could introduce micro-fractures to the facing which subsequently can progress to veneer loss. Veneer wear or fracture may occur but the restoration will not need to be replaced as the tooth remains protected by the metal substructure (O’Connell and Kratunova 2014). Heat sterilisation may cause discolouration of the facing material and the manufacturers advise chemical sterilisation for colour stability.
-

- FIGURE 1 Restored primary molars showing the poor aesthetics of the stainless steel crowns in the smile.

-

- FIGURE 2 Prefabricated full coverage restorations currently available for primary molars in order: stainless steel crown, crown former for composite posterior strip crown, Nusmile veneered SSC, KinderKrown VSSC and a zirconia crown.

-

- FIGURE 3 Provision of a full coverage restoration using the Hall technique. No local anaesthesia or tooth preparation. A. placement of orthodontic separators B. space provided after 1 week C. Cementation of SSC

-

- FIGURE 3

-

- FIGURE 3

-

- FIGURE 4 Life-like aesthetics of pre-veneered SSC (VSSC) placed on the lower first primary molars A. the smile line and B. intraorally

-

- FIGURE 4

-

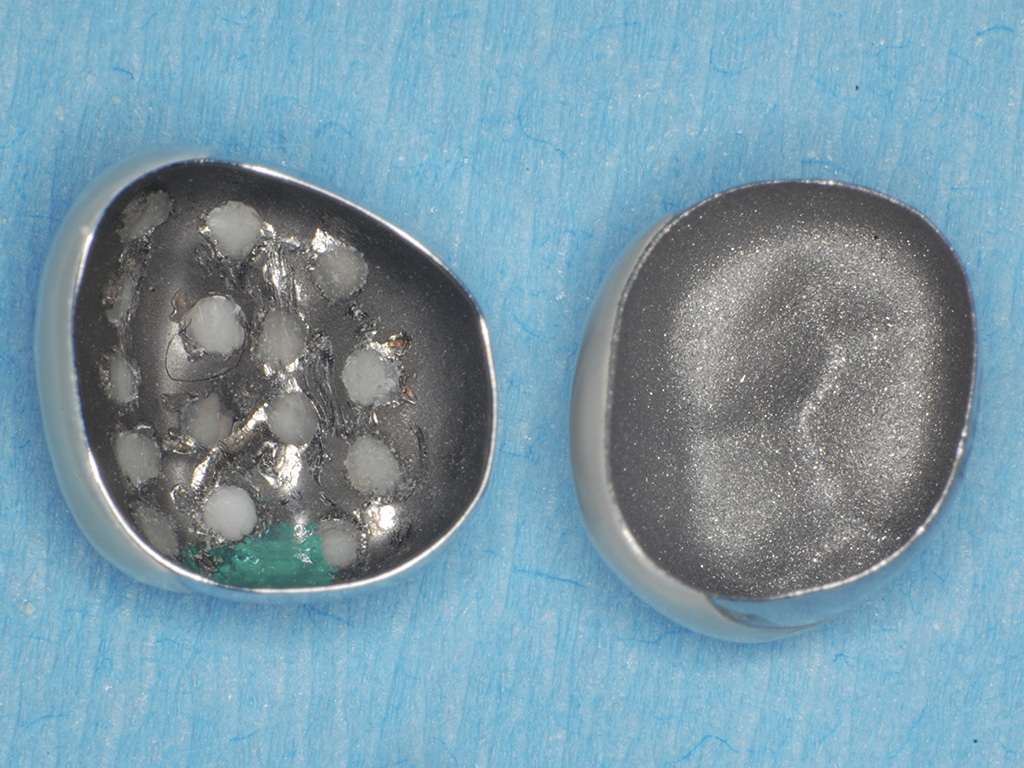
- FIGURE 5 A. The internal surface and B. external surface demonstrating differences between the various commercial brands of VSSC
-

- FIGURE 5

-

- FIGURE 6 Primary molar zirconia crowns A. Excellent aesthetics in the smile B. Intra-oral view of same child

-

- FIGURE 6

-

- FIGURE 7 Variations in the size, contour and anatomy of the various manufacturers of prefabricated zirconia crowns currently available requiring modifications in tooth preparation.
Prefabricated paediatric zirconia crowns
Zirconia has become increasingly popular as a restorative material due to its exceptional properties combining high aesthetic value and excellent mechanical characteristics (Zarone et al. 2010). Prefabricated paediatric zirconia crowns were first manufactured for clinical use in 2007. The solid zirconia construction offers high strength and durability along with superior aesthetics due to realistic anatomy and shade of the crowns (Fig 6a, 6b). It has been demonstrated that zirconia does not enhance bacterial adhesion and growth (Scarano et al. 2004) so that the surface biocompatibility and thin gingival margins of the crowns do not compromise gingival health. The colour of zirconia crowns is stable and fracture of the ceramic is unlikely given the high flexural strength and fracture toughness of the material. These crowns can be used in nickel-sensitive patients.
Zirconia is rigid and must fit passively on the tooth, therefore clinical skill is required to allow for appropriate (but not excessive) tooth preparation. The tooth preparation is critical as no crimping is possible in the zirconia crowns and adjustment of zirconia is not advised. In addition, each manufacturer of zirconia crowns emphasises different anatomical features that will necessitate alteration of the tooth preparation for maximum success (Fig 7).
Local anaesthesia is required for the tooth preparation with occlusal reduction of 1.5 – 2mm. Circumferentially, the primary tooth is reduced uniformly 1.5mm with a subgingival margin extension of 1-2mm. The zirconia crown should have a passive fit without any friction on tooth structure and no bulging of the gingival tissue. Paediatric zirconia crown kits are now commercially available in the EU and are very attractive for patients/parents and clinicians.
There are no published prospective clinical trials published so far reporting on the performance of zirconia posterior crowns, but data on anterior primary teeth shows that they perform well over time.
The general dental practitioner should use full coverage restorations routinely, especially for children with cavitated proximal lesions and in children assessed as high risk for caries. There have been significant advances in restorative paediatric dentistry and the newer options exist to provide aesthetic restorations for children.
The use of Class 2 restorations using composite, compomer, or glass ionomer should be restricted to small proximal lesions in children at low caries risk, or as a temporary solution. Selection of the most appropriate restoration must be based on the individual case and additional training will be required for clinicians to become competent in these techniques.
All these options however are valuable as part of the clinicians’ armamentarium providing restorative choice in the contemporary paediatric dental practice.
About the authors
Anne C. O’Connell, BA, BDentSc, MS, FIDT
Evelina Kratunova, BDentSc, MFD(RCSI), DCh Dent, FFD(RCSI)
References
Engel RJ. Chrome steel as used in children’s dentistry. Chron Omaha Dist Dent Soc. 1950; 13:255-258. Epidemiol. 1998; 26(1 Suppl): 8-27.
Gallagher S, O’Connell BC, O’Connell AC. Assessment of occlusion after placement of stainless steel crowns in children – a pilot study. J Oral Rehabil. 2014 Oct;41(10):730-6. 10.
Guess PC, Att W, Strub JR. Zirconia in Fixed Implant Prosthodontics. Clin Implant Dent Relat Res. 2010 Dec 22.
Hickel R, Kaaden C, Paschos E, Buerkle V, García-Godoy F, Manhart J. Longevity of occlusally-stressed restorations in posterior primary teeth. Am J Dent. 2005 Jun; 18(3): 198-211.
Hosoya Y, Omachi K, Staninec M. Colorimetric values of esthetic stainless steel crowns. Quintessence Int. 2002 Jul-Aug; 33(7): 537-41.
Humphrey WP. Use of chrome steel in children’s dentistry. Dental Survey. 1950; 26: 945-949.
Innes N, Evans D, Hall N. The Hall Technique for managing carious primary molars. Dent Update. 2009 Oct; 36(8): 472-4, 477-8.
Innes NP, Evans DJ, Stirrups DR. Sealing caries in primary molars: randomized control trial, 5-year results. J Dent Res. 2011 Dec;90(12):1405-10.
Kidd EA. How ‘clean’ must a cavity be before restoration? Caries Res. 2004 May-Jun; 38(3): 305-13.
Kindelan SA, Day P, Nichol R, Willmott N, Fayle SA; British Society of Paediatric Dentistry. UK National Clinical Guidelines in Paediatric Dentistry stainless steel preformed crowns for primary molars. Int J Paediatr Dent. 2008 Nov; 18 Suppl 1: 20-8.
Kratunova E, O’Connell AC. A randomized clinical trial investigating the performance of two commercially available posterior pediatric preveneered stainless steel crowns: a continuation study. Pediatr Dent. 2014; 36(7):494-8.
Leith R, O’Connell AC. A clinical study evaluating success of 2 commercially available preveneered primary molar stainless steel crowns. Pediatr Dent 2011; 33:300-6.
O’Connell AC, Kratunova E, Leith R.Posterior preveneered stainless steel crowns: clinical performance after three years. Pediatr Dent. 2014 May-Jun;36(3):254-8
Ricketts DN, Kidd EA, Innes N, Clarkson J. Complete or ultraconservative removal of decayed tissue in unfilled teeth. Cochrane Database Syst Rev. 2006 Jul 19; (3): CD003808.
Scarano A, Piattelli M, Caputi S, Favero GA, Piattelli A. Bacterial adhesion on commercially pure titanium and anatase-coatedtitanium healing screws: an invivo human study. J Periodontol. 2010 Oct; 81(10): 1466-71.
Seale NS, Randall R The use of stainless steel crowns: a systematic literature review. Pediatr Dent. 2015 Mar-Apr;37(2):145-60
Thompson V, Craig RG, Curro FA, Green WS, Ship JA. Treatment of deep carious lesions by complete excavation or partial removal: a critical review. J Am Dent Assoc. 2008 Jun; 139(6): 705-12.
Verifiable CPD Questions
AIMS and OBjectives:
- To introduce the concept of aesthetic dentistry for children
- To explain the various options for prefabricated crowns for primary molars
- To describe the differences between the types of crowns
- To encourage general dental practitioners to use prefabricated crowns.
LEARNING OUTCOMES:
- To understand the variety of alternative restorations that increase the scope of their professional practice
- Understand the options available for restoration of primary molars
- To become familiar with the essential steps for tooth preparation.
Example question:
The correct position of the crown margin in a primary molar is:
A. At the gingival margin
B. Sub gingival
C. Supragingival
D. Location dictated by extent of caries.
1 Comment
Does anyone know of any dentist(s) in the UK who actually use prefabricated paediatric zirconia crowns? I would like this as a nickel-free alternative for my 5-year-old but have only been able to find practitioners in US and Australia.