Decontamination – where are we now?
The decontamination of dental instruments is a vital element of any general dental practice. Irene Black gives an update on the current situation

Like most topics, decontamination has gone through phases of being high profile and then seemingly disappears off the radar. Recently, when decontamination does re-emerge, it is often when errors or omissions have been identified. It is still undoubtedly an extremely emotive issue, particularly when things go wrong. It is also a critical element as far as patient safety is concerned.
Dental practices and their teams have come a long way in the last five years as far as decontamination is concerned. We have been in a period of consolidation as far as guidance and requirements are concerned but, in my experience, we occasionally slip back into old habits. Reviewing and refreshing our knowledge and skills is essential to ensure we are following the requirements and able to show we are doing the right things to the best of our ability.

Figure 1
The decontamination cycle (Fig 1)
Decontamination is the process by which reusable items are rendered safe for further use on patients and safe for staff to handle. The process is complex and involves several stages, with potential for error throughout.
The decontamination cycle begins in the surgery with segregation of reusable items and disposal of single-use items and other materials in appropriate waste containers. Items to be processed for reuse must be transported safely to the Local
Decontamination Unit (LDU) as soon as possible. The transport boxes should be rigid, lidded, and easy to clean. These transport boxes must be easily identifiable as containing either ‘dirty’ or ‘clean’ items to avoid any potential confusion. Colour coded boxes are often the simplest way to ensure this. Using marker pens or labelling only the lids still leaves potential for error.
The next stages of the cycle are cleaning, inspection, sterilisation packing and storage.
Local Decontamination Units (LDU)
Dental practices today – space, the first frontier
Today, those considering setting up new dental practices need to make sure they have enough space to meet current requirements and ensure they are future proofing their setting. Recently, the number of dental professionals looking to set up new practices has been increasing. The settings of choice tend to be small commercial units in shopping areas where there is potential for patient footfall. I do have some concerns that, in the drive for financial viability, they are starting out with a limited area and will find they run out of space in a short time.
Despite advances in new technology, implying that practices should become more streamlined, the reality is we have many more items to house. In my experience, our need for storage capacity has not decreased despite the drive towards paperless systems and digital advances. Lack of space can result in cluttered, chaotic and disorganised settings with less potential to create a good impression and more potential for error, particularly in relation to good infection control and decontamination.
LDU compliance
Current guidance states an LDU compliant with SHPN13 is essential for primary care dental practices (Compliant Dental Local Decontamination Units in Scotland (Primary Care) (2013)).
Key points
General requirements for LDUs:
- Away from the clinical area and no activity other than decontamination undertaken
- Dirty and clean areas clearly demarcated
- Instrument flow from dirty to clean
- Smooth cleanable surfaces
- Well lit with ventilation
- Enough space for equipment and set-down areas.
Essential components
- Hand wash sink and Personal Protective Equipment (PPE)
- Set-down areas
- Washing sink and rinsing sink
- Washer disinfector
- Inspection areas
- Sterilisers
- Packing area.
Every dental practice in Scotland now has a room dedicated to the decontamination of dental instruments. Having an LDU is the accepted norm and is an essential requirement for the Combined Practice Inspection. These LDUs can undoubtedly vary in shape and size, but the general lay out should be in line with the single room model as stipulated in Scottish Health Planning Note 13 (SHPN13). There are sometimes some minor variations in the configuration and they may not all follow the exact requirements of SHPN13.
The design differences often relate to limited space available or build decisions determined by a contractor. Limitations such as plumbing, or other seemingly insurmountable building difficulties, have often been identified as the cause. In some cases, health boards may have agreed to minor deviations from the guidance to ensure continuance of a service when there appeared to be no other option available.
Some LDUs are undoubtedly smaller than the preferred option and space constraints are not ideal. In these circumstances, it is essential that the correct process is applied to the letter every time to avoid errors. These errors are often due to insufficient set-down space. All staff must be trained accordingly to ensure everyone knows and follows the exact procedures in place for that setting.
Other difficulties relate to using the dedicated LDU for other purposes. Again, this usually comes about due to overall space limitations in the practice. These other activities have ranged from housing X-ray developers to tea and even food preparation, neither of which is acceptable either for staff or patients. Hopefully, that message has been heard loud and clear and common sense now dictates that this is not acceptable.
LDUs are now in use across Scotland. Staff have accommodated remarkably well. I don’t believe many would wish to go back to carrying out decontamination in the clinical area. The constant background activity of washing up, while an ultrasonic rattled incessantly and autoclaves generated sauna-like conditions, was not exactly conducive to the provision of good quality patient care.
-

- FIGURE 2A SHPN 13 part 2 Dedicated separate Room/rooms
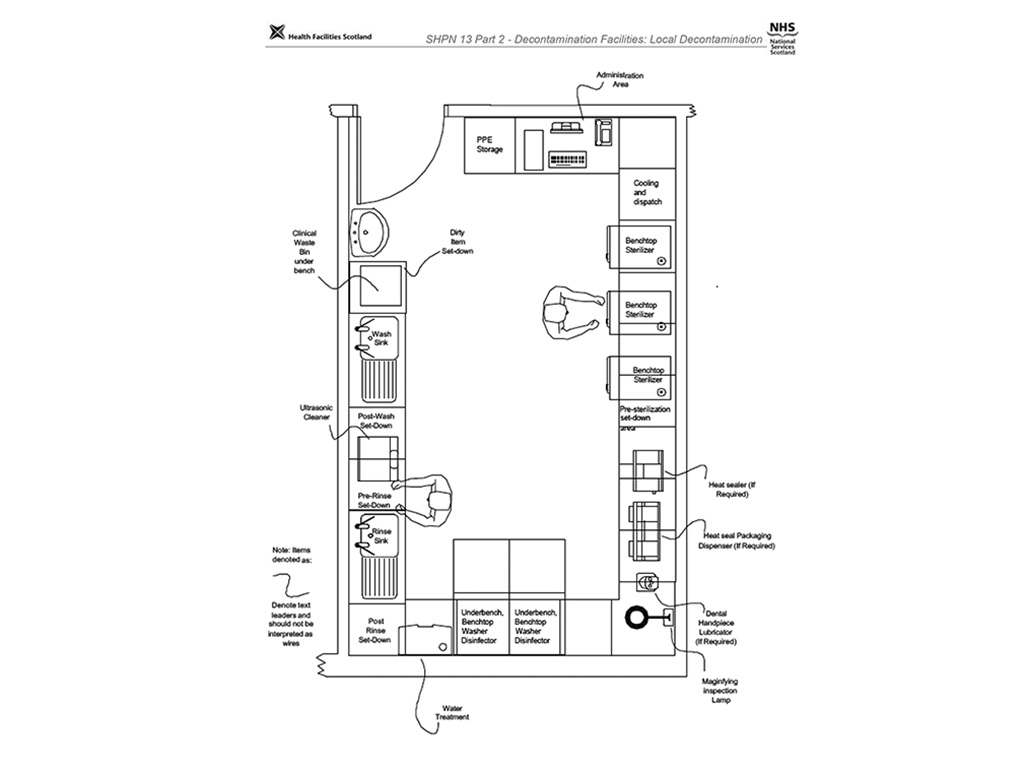
-

- FIGURE 2B Washer disinfector in LDU

-

- FIGURE 3 single-use symbol

-

- FIGURE 4 clip trays

-

- Tray of instruments loaded correctly for optimal processing in a non-vacuum steriliser
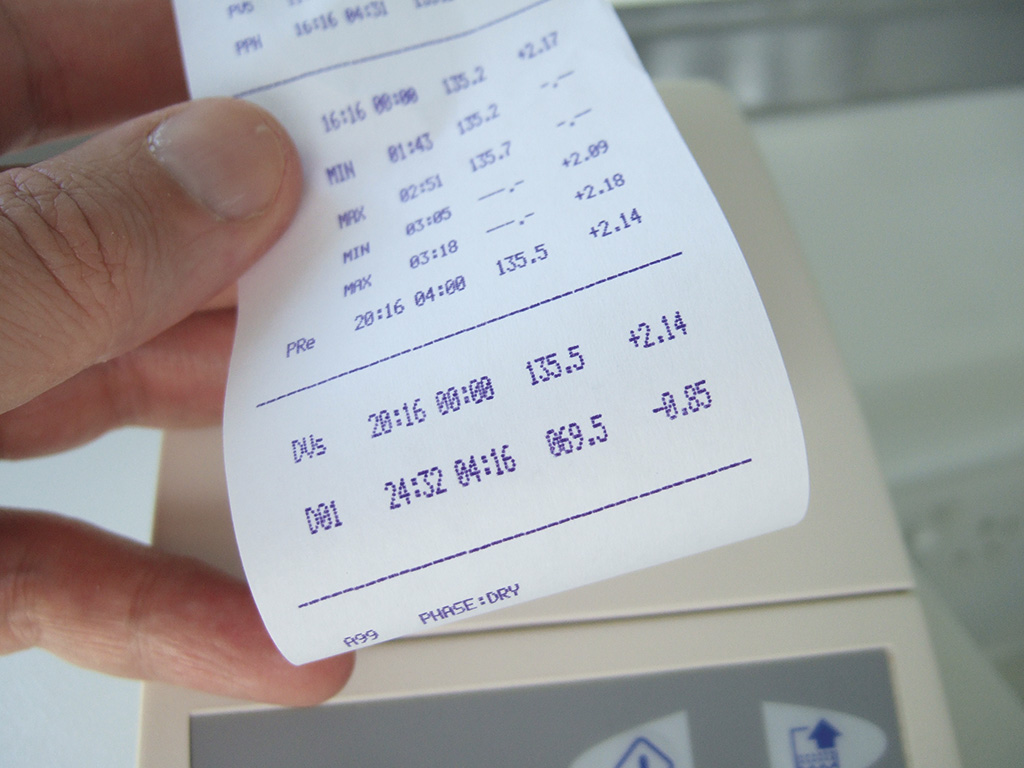
-

- Print-out showing the parameters reached during the sterilisation cycle
Single-use items
The guidance stipulates that the use of single-use items should be the option of choice where possible as long they are viable and work effectively for the purpose required. All items carrying the single-use symbol (Fig 3) should not be re-used or reprocessed. If this symbol appears on an item this is part of the manufacturer’s instructions. Compliance with manufacturer’s instructions is accepted as the legal requirement for all equipment.
Specific single-use items that have presented difficulties include:
- Three-in-one tips. Reusable metal tips are unacceptable as they are extremely difficult to clean and there are good disposable alternatives. The requirement for single use three-in-one tips is part of the practice inspection.
- Endodontic files. This has been a requirement in Scotland since 2004 and has not changed. (The situation in England is different in that they allow for re-use on the same patient. The issue with this is the exacting requirement for reprocessing and the potential for error as far as identification and storage are concerned.)
- Plastic impression trays are single-use despite the fact labs return them to practices for disposal. The effort required to clean and re-use most certainly outstrips any benefit gained considering the time and energy expended on trying to clean and prepare these for re-use.
- Matrix bands. There is evidence to show that these items, which are often heavily
contaminated with blood, cannot be cleaned effectively and present a risk to staff and patients. These must be dismantled with care and disposed of in appropriate waste containers for sharps. The holder must then be cleaned and sterilised. There are single-use alternatives.
The decontamination process
The decontamination process is about the application of knowledge and skills and is dependent on what individuals do in their own settings. The decontamination process in the LDU includes cleaning, inspection, sterilisation and packing for storage.
The general principles of the process are:
- All items should be processed according to manufacturer’s instructions. The problem with this can be that the instruction provided may not be clear or explicit. In that case, you are entitled to request information from the manufacturer or via the supplier.
- The flow of the instruments in the decontamination process is always from the dirty to clean area and never goes back in the process. The only exception would be if visible soil is picked up through inspection and the item is returned to the start of the cycle to repeat the full process.
- Using an automated cleaning process is required and washer disinfectors are essential for cleaning dental instruments.
- All re-usable items must be at least sterilised if not sterile at the point of use.
- Policies and procedures must be in place for all aspects of decontamination. All staff must have read these and can access them for easy reference.
Cleaning
Washer disinfectors – the final hurdle for compliance?
“Use of a washer disinfector (WD) is a requirement for compliant reprocessing of dental instruments” (Compliant Dental Local Decontamination Units in Scotland (Primary Care) (2013)). Using a washer disinfector is the preferred method for cleaning dental instruments because it offers the best option for the control and reproducibility of cleaning. This means the cleaning process can be validated. WDs are used to carry out the processes of cleaning and disinfection consecutively.
A typical WD cycle for instruments includes the following five stages:
- Flush – Removes gross contamination. Latest standards indicate that a water temperature of <45°C is used to prevent protein coagulation and fixing of soil
to the instrument - Wash – Removes any remaining soil. Detergents used in this process must be specified by the manufacturer as suitable for use in a WD
- Rinse – Removes detergent used during the cleaning process.
- Thermal disinfection – The temperature of the load is raised and held at the pre-set disinfection temperature for the required disinfection holding time: for example, 80˚C for 10 minutes, or 90˚C for one minute
- Drying – heated air removes residual moisture. Some manufacturers have worked on this in an effort to reduce cycle times as this was a significant barrier to their use. They have endeavoured to reduce the cycle times to improve efficiency for use in practice and while still demonstrating effective cleaning efficacy as per testing requirements.
What have the problems been?
It is safe to say that the dental profession in Scotland has been slow to adopt this piece of equipment as a ‘must have’ as they strive towards best practice in decontamination.
The reasons for this are varied and complex. The reputation of these items have been somewhat tarnished often through anecdote and bad press. Admittedly, this was not helped by some genuine technical problems related to specific machines resulting in some practitioners experiencing difficulties despite their best efforts. Negotiations with suppliers and manufacturers have been ongoing in an effort to resolve specific cases. From the outset, some practitioners heard about these problems and simply decided not to try for themselves.
Another difficulty with washer disinfectors was that they didn’t fit naturally and seamlessly into our existing processes. We had to change aspects of what we did to make them work efficiently and effectively for us. Change is difficult and it takes time. The early abandoners ran out of patience and gave up quite quickly. Some of the more tenacious teams persevered and have become converts. Recently, I have had some surprisingly positive feedback from some of the more strident early objectors.
The fact is, these machines are an essential requirement in Scotland to ensure our reusable instruments are clean and able to be sterilised effectively.
To utilise a washer disinfector efficiently and effectively, in my opinion, we need several things. First of all, you need have done a capacity calculation to work out which washer disinfector suits the needs of your practice. The overarching aim is ultimately to run the washer disinfector a minimum number of times a day and only put it on when it’s at or close to its full capacity. To work that out, you need to look at:
- How many items are used in the practice in an average session?
- What does the WD hold?
- Could the internal set-up be improved to hold more?
- How long will it usually take to get the WD to capacity?
- How long does the full decontamination cycle take?
- Do you have enough stock of instruments to avoid shortages at busy times?
In my opinion, using clip trays (Fig 4) for cons kits are essential to allow the WD to work efficiently for you. The initial capital outlay will save running cost in the longer term. It also reduces risks for staff having to spend time dismantling open trays, which need to cleaned separately and then reassembled before storage.
Members of the dental team who work in the LDU are best placed to work this out and establish a routine that suits the way the practice works and use the WD efficiently and effectively.
Ultrasonic cleaners
Compliant ultrasonic cleaners are also an automated cleaning method. They are useful as a back-up cleaning method. They are no longer an essential requirement as far as the practice inspection is concerned as washer disinfectors are the first line cleaning method and an essential requirement.
Ultrasonic cleaners can be utilised to pre-clean particularly heavily soiled instruments before processing in the washer disinfector. This is useful if there is a delay before the washer disinfector is at capacity and heavily contaminated surgical kits would become difficult to clean if left to dry out. Pre-cleaning is advisable in that situation.
Using an ultrasonic cleaner if the washer disinfector is down for short periods is acceptable. The ultrasonic cleaner will have to be validated and tested as per manufacturers’ instructions to ensure it is functioning effectively if it has to be brought back into use. In a busy practice, an ultrasonic alone may not provide the capacity required to ensure throughput and it may be necessary to revert to full manual cleaning as well.
Reverting to full manual cleaning utilises significant volumes of hot water,
detergent and staff time. It also puts your staff at risk of injury. Using manual cleaning should only be adopted as a last resort for cleaning dental instruments. When service and maintenance contracts for washer disinfectors are being arranged some assurance from the supplier as to their response time and contingency plans, if the washer disinfector fails, should be sought. Details of full manual cleaning process can be found in The SCDCEP guidance document – Cleaning Dental Instruments, can be accessed at www.sdcep.org.uk/published-guidance/decontamination/
Handpieces and washer disinfectors
Cleaning handpieces effectively due to the extremely narrow lumens is a difficulty. As far as I am aware, there has been little progress on effective handpiece cleaning in washer disinfectors. Some practices are processing handpieces in their washer disinfectors without detriment to their equipment. Most practices are understandably tentative about putting these delicate, expensive items in their washer disinfector. There is no specific guidance that stipulates this is a requirement. If you plan to process handpieces in a washer disinfector, make sure you have written instructions and an assurance of compatibility from both the handpiece and the washer disinfector manufacturer.
Decontamination process – sterilisation
All reusable items must be sterilised. From time to time we come across situations where there is some confusion as to what type of autoclave is in use or which cycle is being used. It is imperative that the whole dental team understands the difference between vacuum and non-vacuum cycles in benchtop sterilisers to ensure these are used safely and effectively.
- A non-vacuum cycle can only be used for unwrapped items. When the cycle is complete, the items will have been sterilised.
- It is essential that any steam steriliser is not overloaded.
- If a vacuum cycle is used, items can be wrapped or bagged before sterilisation. When this cycle is complete, the items will be sterile as long as the packaging is intact.
Please note, if items are wrapped before being placed in a non-vacuum cycle. they will not have been sterilised. If these items were subsequently used. this presents a significant risk to patient safety. This is a serious event and must be reported.
Maintenance, testing and validation of all decontamination equipment
There tends to be some confusion as to what is required as far as testing and validation of equipment is concerned and what your engineer, supplier or manufacturer provides as part of contractual arrangements.
Maintenance contracts for your decontamination equipment are required to make sure the equipment is in good mechanical working order. You may have options as far as the cover you choose. Make sure you are certain which cover you are paying for and exactly what it includes. Testing and validation are not the same as general maintenance. Your engineer may do this at the same visit as part of the contract. Always make sure you know exactly what they have carried out and retain all paperwork as evidence.
Validation is a documented procedure used to show that the decontamination process will repeatedly and consistently take place to a satisfactory standard when defined operating conditions are used. Validation checks and tests are carried out at least annually, which is referred to as revalidation. Some manufacturers may refer to this as annual testing rather than revalidation.
Periodic testing is required to ensure that WDs perform consistently as specified at validation.
Tests and testing intervals will be stipulated in manufacturer’s instructions. Some of these tests will be carried out by practice personnel and provide regular checks to evidence that equipment is operating as per the parameters determined at validation.
A test person (engineer) will carry out periodic testing/revalidation as specified in the manufacturer’s instructions. This will be required at least annually. Always check with your engineer and make sure you know what is being carried out at each visit.
Testing carried out by practice teams include:
- Automatic control tests. These are required for washer disinfectors, ultrasonic baths and autoclaves. Details on how to perform automatic control tests can be found in the SDCEP decontamination guidance: www.sdcep.org.uk/published-guidance/decontamination/
- Cleaning efficacy tests are used to demonstrate the ability of washer disinfectors and ultrasonic baths to remove soil and contamination. Consult your manufacturer to see which tests are recommended and how often these should be done.
Storage
As far as storage of dental instruments after sterilisation is concerned, the general principle for all reusable items is to ensure that the potential for re-contamination through direct contact or aerosol production is eliminated.
Aerosol production during clinical procedures presents a risk of contamination of surfaces and items within the area. Aerosols contain blood, saliva and significant levels of associated micro-organisms. This can constitute a risk of transmission of infection as many of these micro-organisms can survive on surfaces for variable periods of time. Thorough environmental cleaning and closed storage must be applied to avoid potential risk of transmission of infection.
The practice of bulk storage of items for intraoral use should be discontinued. Using drawer inserts to store loose mirrors and probes is not acceptable as far as avoiding possible contamination is concerned. Storage options include the bagging of examination and other kits. Bagging of forceps and other items for oral surgery has been accepted as the norm for some time. Conservation kits in clip trays should be stored covered with a lid or bagged and can be placed in cupboards in racks or drawers either in the clinical area or in a central storage area.
All items for clinical procedures should be set out for use on each patient immediately before the treatment episode. During clinical procedure, when extra items stored in drawers or cupboards are required, good local systems for retrieval to avoid potential contamination of other items must be in place. This may involve glove removal and use of clean tweezers to ensure efficient safe practice.
Practices may have adopted different ways of fulfilling the requirements for storage related to their specific storage spaces and practice layout. Avoiding the potential for recontamination is essential and should be considered fully to ensure there are safeguards to ensure the risk of this is eliminated as far as possible.
In general:
- No unnecessary items intended for clinical use should be set out on work surfaces during clinical procedures. Reduced clutter means easier cleaning.
- Items set out for a specific patient treatment and not used must be fully reprocessed or disposed of if single use.
- Sterilised items even in closed storage such as cupboards or drawers should be covered.
There is no specific guidance in Scotland as far as the timescale for safe storage of non-sterile or sterile items. HTM 0105, the guidance applied in other areas of the UK apart from Scotland, stipulates more exacting requirements for storage (click here to see PDF)
Training
The need for suitable training enabling the application of good infection control and decontamination, in line with Scottish guidance, is essential for the whole dental team. Another essential requirement is quality assurance. Audit is the accepted method of choice. This is essential, not only for infection control purposes, but also to fulfil NHS terms of service.
NHS Education for Scotland can provide both and help to avoid the pitfalls.
Our national infection control support team is made up of dental nurses with extensive experience both in practice and as trainers. They have been trained specifically to Scottish infection control and decontamination guidance requirements. They have a wealth of knowledge and are fully aware of the differences in guidance in others parts of the UK. Our team can tailor sessions to meet any needs the practice feel they have. For example. if you are struggling to integrate your washer disinfector into your usual process. our team can help.
The training does provide knowledge, but the real focus is on practical application. In a busy practice, knowing what to do doesn’t mean we all do it every time. Our sessions are designed to identify what makes the application of that knowledge challenging and what might help to make that change. Providing the practice with an action plan is an essential element to enable these changes. This plan will be supported and followed up. We also have two short e-learning programmes that are useful for updates or induction for new staff. These can be accessed though the NHS Education Portal (https://portal.scot.nhs.uk/)
On request, in conjunction with booking a training session, dentists can access four pre-populated audits via the NES Portal covering four areas of infection control and decontamination. Our team can review data collection and provide feedback on audit reports. After submission of a satisfactory report, dentists will have evidence of quality assurance in their practice and be eligible for audit hours and allowance.
NHS Education for Scotland has worked hard over the last years to ensure a consistent message based on Scottish guidance requirements has been delivered to the whole dental team in every practice in Scotland. NES has delivered 2,313 in practice training sessions to 6,511 dentists and 1,335 DCPs.
The message is out there. If you feel your team could benefit from our training, please contact Natalya.Zhernakova@nes.scot.nhs.uk or call 0141 352 2642.
About the author
Irene Black graduated from Glasgow University in 1980, gained her Membership of the Faculty of General Dental Practitioners in 1999 and the Certificate in Effective Dental Management in 2005.
Along with her husband, she owned an NHS dental practice in Eaglesham for 27 years where she continues to work on a part-time basis.
Irene has been a dental practice adviser in Greater Glasgow and Clyde health board for 14 years and her interest in education developed during nine years spent as a vocational trainer.
She has worked as an assistant director for NHS Education with the remit for infection control and decontamination for the last eight years. This has included developing both in-practice and other training packages for the dental team. As part of this role, she has worked with Scottish Government and other NHS organisations in an effort to determine how the difficulties related to decontamination in dental services might be resolved.
Irene also works with the Scottish Dental Clinical Effectiveness Programme in guidance development and research.
References
Scottish Health Planning Note 13 Part 2, Local Decontamination Units (www.hfs.scot.nhs.uk/online-services/publications/decontamination/)
Local Decontamination Units: Guidance on the Requirements for Equipment, Facilities and Management (www.documents.hps.scot.nhs.uk/hai/decontamination/publications/ldu-001-02-v1-2.pdf)
Compliant Dental Local Decontamination Units in Scotland (Primary Care) (2013) (http://www.hfs.scot.nhs.uk/publications-1/decontamination/)
Verifiable CPD Questions
Aims and Objectives:
This article reviews the general principles of decontamination and highlights some aspects that have been challenging for dental practices and their teams.
LEARNING OUTCOMES:
After reading this article you should be able to:
- Plan the general layout of a single room local decontamination unit.
- Describe each stage of the decontamination cycle.
- Demonstrate the decontamination process in your own setting
- Discuss the testing requirements for decontamination equipment.
- Identify the relevant guidance documents for decontamination in Scotland.
Dental practices and their teams have come a long way in the last five years as far as decontamination is concerned
Submit your answers listings
Comments are closed here.