
A risky business?
Patients with periodontal problems can present particular challenges when carrying out advanced restorative work

Demand for dental implants is growing and patient acceptance of removable appliances is lower than in the past, as those who can afford to pay request restorations that are “fixed” in their jaws. Much of this demand, especially when multiple tooth replacement is considered, is from patients with a history of, or ongoing, periodontal problems.
This demand brings its own set of challenges, as many of the factors which put patients at risk of periodontitis and ongoing bone loss around teeth seem to apply to implants. What we are doing for many of these individuals is moving them from a state where periodontal disease has compromised tooth retention, one which they and their dentists have been unable to control, to a situation where they have complicated and expensive restorations, which need high degrees of skill to maintain, and which are susceptible to similar challenges in the medium and long term.
Our challenge as professionals advising and caring for these patients is to understand this and to plan and execute treatments to take their history into account. How can we reduce the likelihood that patients who had periodontitis, which caused them to lose their teeth prematurely, don’t suffer the same fate five, 10 or 15 years down the line after they have implants placed?
Loss of implants often leaves large tissue defects, which can be extremely challenging to restore at a later date
The aim of this article is to outline periodontal considerations when planning for successful restorations and working with this challenging group of patients.
Risk assessment
In long-term studies looking at implant retention, patients with periodontitis affecting their natural dentition were more at risk of developing problems in an implant restored one, whether or not they retained some natural teeth1,2. Current research seems to support the contention that implants will fare less well in patients with a history of aggressive periodontitis3,4. These problems become more pronounced with time1 and apply not principally in terms of absolute survival but in terms of problems which require intervention but may not result in implant loss, e.g. peri-implantitis. Key to success for patients with periodontal problems who are considering implants is assessing and then reducing this risk5.
Using historical evidence relating to periodontitis in an individual can be a valuable assessment tool in terms of potential ongoing risk. This is done by considering the history with regard to periodontal disease and the presence of additional risk factors6, which may contribute to implant-related problems.
For the purposes of this assessment, a thorough periodontal history and examination is required.
History
In the patient history the following factors may be indicative of higher risk:
- Smoking
- Systemic factors, particularly diabetes and stress
- Family history of early tooth loss that is related to periodontal disease
- History of tooth loss secondary to periodontal problems
- Poor outcomes of previous periodontal treatments.
Examination
In patients with complicated disease, as displayed by increased BPE scores, this examination will involve a full six-point pocket chart as well as an assessment of levels of oral hygiene and gingivitis. Radiographs should be assessed for the presence of periodontal bone loss (Fig 1).
Periodontal examination will highlight levels of periodontal attachment, the presence of areas of inflammation (as observed by bleeding on probing), areas of infection (suppuration on probing) and levels of tooth mobility. This thorough assessment enables the clinician and patient to understand the level of disease present, quantify risk of inflammatory breakdown and plan comprehensively for potential restorations at an early stage.
Donos et al7 categorised patients as low, medium and high risk for implant placement partially on the basis of these combined periodontal risk factors and clinical examinations:
High risk (Fig 2)
- Presence of aggressive or refractory periodontitis
- High plaque and bleeding on probing scores
- Smoking
- Systemic factors e.g. diabetes.
Medium risk (Fig 3)
- Previous periodontal disease overall successfully treated but still limited number of residual pockets >5mm and less than ideal oral hygiene.
Low risk (Fig 4)
- Systemically healthy
- Good response to periodontal therapy and displaying optimal oral hygiene
- Non-smoker.
Treatment modality selection
One of the fundamental questions when planning for this group of patients is the question of when to retain or extract teeth. The essential question is: will implants fare better, or even as well as, teeth in the medium and long term for the high-risk patient? A reasonable starting point may be that implants are a replacement for no teeth rather than a replacement for teeth.
Prior to removing teeth it is sensible to consider whether the patients’ own natural implants, their teeth, could be retained by a specialist rather than be extracted. Many long-term studies8,9 have shown that, following good-quality periodontal treatment and stabilisation of the periodontal tissues, it is possible to retain even severely compromised teeth for long periods of time.
This retention involves high degrees of skill and diligence by patients and support on a regular basis from a dental professional. However, this degree of required ongoing maintenance is not different with implants. Indeed, it is often much easier to maintain teeth than implant-supported restorations when one considers the morphology of restorations and the rough nature of many implant surfaces.
In high-risk patients, Donos et al.7 suggested that implants should not be provided and, instead, that maintenance of teeth should be a priority and restoration based on removable and conventional dental restorations supported on teeth rather than implants. This concept challenges opinion when one considers that many perceive removal of teeth and placement of implants as a good option for periodontally compromised teeth.
Of course, the decision to remove teeth is not purely periodontal, often due to compromised aesthetics following periodontitis, for example drifting of anterior teeth, or as a result of other restorative failure a decision is made to remove teeth. This is often, in fact, what patients request. Even in these cases the long-term consequences of removing teeth and rebuilding an aesthetic replacement, which will have to be retained and maintained, need to be carefully discussed with the patient. Loss of implants often leaves large tissue defects which can be extremely challenging to restore at a later date.
-

- Figure 1 – Radiographic presentation of aggressive periodontitis

-

- Figure 2 – Clinical features of aggressive periodontitis; high risk for implant restorations

-

- Figure 3 – Controlled chronic periodontitis and good maintenance; medium risk for implant restorations

-

- Figure 4 – Patient with external resorption of central incisor, no evidence of periodontitis, good OH and non smoker; low risk for implant restorations

Patient preparation
If the decision has been made to provide an implant-retained restoration for a patient with a history of periodontitis, it is vital that the patient is fully prepared for the procedure.
Patients should understand what will be required to maintain their restoration and prosthesis design should be discussed in terms of the ease of maintenance of a fixed versus removable, semi-fixed option. They should be given the opportunity to learn the skills needed to maintain their restoration prior to the uncomfortable post-surgical phase that challenges them in this respect. If patients are having a mixed restoration, i.e. retained teeth and implants, these skills can be acquired around natural teeth (Figs 5-10).
In this preparation phase we are essentially trying to accomplish several things:
- Turn a previously “bad” patient, one who has lost teeth secondary to disease, into a “good” one, where disease is controlled and burnt out and the patient’s risk is substantially reduced by their changed habits – i.e. good and regular OH, smoking cessation and attendance for regular and tight maintenance
- Establish conditions of periodontal health which reduce the risk to implants in the medium and longer term
- Allow the dentist some time to assess more fully what can and should be done to best restore the dentition. It may be possible to save teeth or a clearer picture may emerge as to what sort of restoration is best, if at all. Many patients function well on the shortened dental arch and the maintenance requirements are low.
Control of periodontitis
If patients have existing periodontitis, this should be controlled prior to implant placement. The aim is to reduce the risk of post-implant placement problems by reducing the likelihood of future periodontal problems. In practice, we should aim for:
- Probing pocket depths below 6mm
- High standard of oral hygiene
- Minimal BOP
- No pus on probing
- Smoking cessation
- Compliance with a regular supportive maintenance programme.
In a dentition where teeth are planned for retention, this will involve well-executed, non-surgical periodontal therapy10,11 but, in more severe cases, may mean that specialist periodontal treatment is needed during that first phase. In many cases specialist periodontal treatment can save teeth which may be deemed hopeless and the need for implants reduced8.
If that is the case then this should be accessed at an early stage to allow for healing of soft tissues and stabilisation of gingival margins prior to restoration. In patients who are to have all teeth extracted it is still worth investing time prior to extractions to control levels of inflammation and improve oral hygiene as a platform for future maintenance of implants12.
Every patient is, of course, an individual but in general terms early periodontal treatment and stabilisation involves:
- Discussion with the patient of aetiology of periodontitis, their risk profile and the effect that may have on implant restorations
- Extraction of teeth with a hopeless prognosis and arrangements for transitional restorations
- Liaison to control any systemic factors contributing to increased tissue breakdown
- Establishment of high levels of oral hygiene as monitored in the medium term, on an objective basis
- Support for smoking cessation
- Scaling to remove supragingival calculus and ease OH
- Sub gingival instrumentation to provide clean, bio-compatible root surfaces and allow the establishment of healthy periodontal support
- In some cases antibiotics may be required if the patient has a more aggressive form of disease
- Opportunity to further discuss with the patient ongoing maintenance requirements and establish habits of attendance for supportive treatment around implants.
If pockets are persistent after non-surgical treatment then principle options will be:
- Surgery for pocket reduction prior to implant placement
- Extraction of non-responding teeth and incorporation into the planned restoration
- Tooth retention and the postponing or cancelling of implant work either until the tissues have stabilised at a later stage or altogether if control is not possible.
Consolidation after this pre-surgical phase allows the clinician to understand better what the longer-term outcome for the patient is likely to be. Any restorations subsequently planned are therefore more predictable. Cancelling or delaying planned implant work is disappointing, however it may be the best option for some patients where periodontitis is not fully controlled. Conventional restorations are less expensive and are often easier to adjust and add to if teeth fail at a later date. This may be the case particularly for those who are have multiple high-risk indicators, e.g. smokers or those with poorly controlled diabetes.
Prosthesis planning
When planning the prosthesis for a patient who has had periodontitis in their natural dentition, the priorities should be to:
- Allow ease of access for good oral hygiene
- Ensure retrievability of restorations so that implant fixtures can be directly assessed and maintained on a regular basis.
The following factors should be considered:
- Removable or fixed
Retrievable restorations are a good option as they allow for maintenance of periodontal tissues by patients and professional staff. This ability to remove a prosthesis and examine tissues directly gives reassurance that implants can be comprehensively inspected and, if problems occur, they can be addressed swiftly.
In terms of how this may be managed, restorations can be removable by patients, as is the case with e.g. a locator-supported denture, allowing for daily plaque control, or screw-retained and removable by the clinician for maintenance, perhaps annually or biannually. Cemented restorations are often used to allow for correction of implant angulation and to avoid screw holes in positions which are aesthetically compromising.
This type of restoration, as well as running the risk of excess cement around the fixture head and “peri-cementitis”13, is extremely difficult to remove for routine maintenance without destroying the superstructure. Unless the patient can adequately access the peri-implant tissues, a cemented design will make maintenance extremely challenging.
-

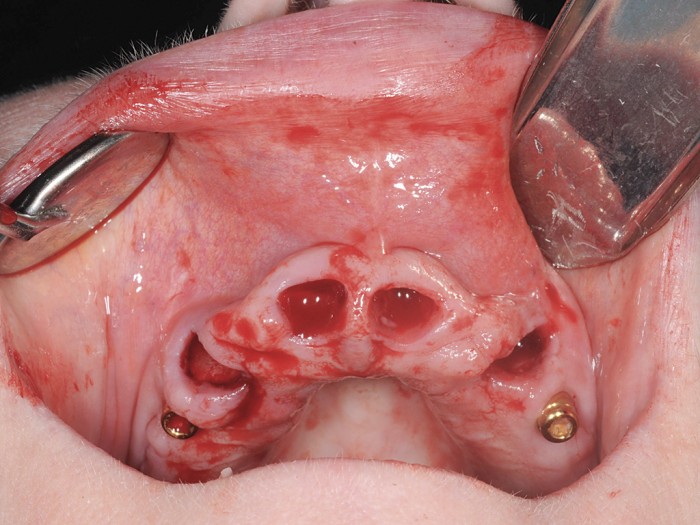
- Figures 5-10 56-year old female presenting for implants. Long-standing severe periodontitis leading to multiple previous tooth loss. Staged approach to treatment tackling periodontal disease and extracting hopeless teeth at an early stage. Adhesive bridge placed in the lower anterior region. Once inflammation stabilised and probing pocket depth reduced, upper teeth extracted in stages and implants placed. Plan in place for an overdenture to allow for easy long-term maintenance of the upper arch
-

- Figures 5-10 56-year old female presenting for implants. Long-standing severe periodontitis leading to multiple previous tooth loss. Staged approach to treatment tackling periodontal disease and extracting hopeless teeth at an early stage. Adhesive bridge placed in the lower anterior region. Once inflammation stabilised and probing pocket depth reduced, upper teeth extracted in stages and implants placed. Plan in place for an overdenture to allow for easy long-term maintenance of the upper arch

-

- Figures 5-10 56-year old female presenting for implants. Long-standing severe periodontitis leading to multiple previous tooth loss. Staged approach to treatment tackling periodontal disease and extracting hopeless teeth at an early stage. Adhesive bridge placed in the lower anterior region. Once inflammation stabilised and probing pocket depth reduced, upper teeth extracted in stages and implants placed. Plan in place for an overdenture to allow for easy long-term maintenance of the upper arch

-

- Figures 5-10 56-year old female presenting for implants. Long-standing severe periodontitis leading to multiple previous tooth loss. Staged approach to treatment tackling periodontal disease and extracting hopeless teeth at an early stage. Adhesive bridge placed in the lower anterior region. Once inflammation stabilised and probing pocket depth reduced, upper teeth extracted in stages and implants placed. Plan in place for an overdenture to allow for easy long-term maintenance of the upper arch

-
- Figures 5-10 56-year old female presenting for implants. Long-standing severe periodontitis leading to multiple previous tooth loss. Staged approach to treatment tackling periodontal disease and extracting hopeless teeth at an early stage. Adhesive bridge placed in the lower anterior region. Once inflammation stabilised and probing pocket depth reduced, upper teeth extracted in stages and implants placed. Plan in place for an overdenture to allow for easy long-term maintenance of the upper arch
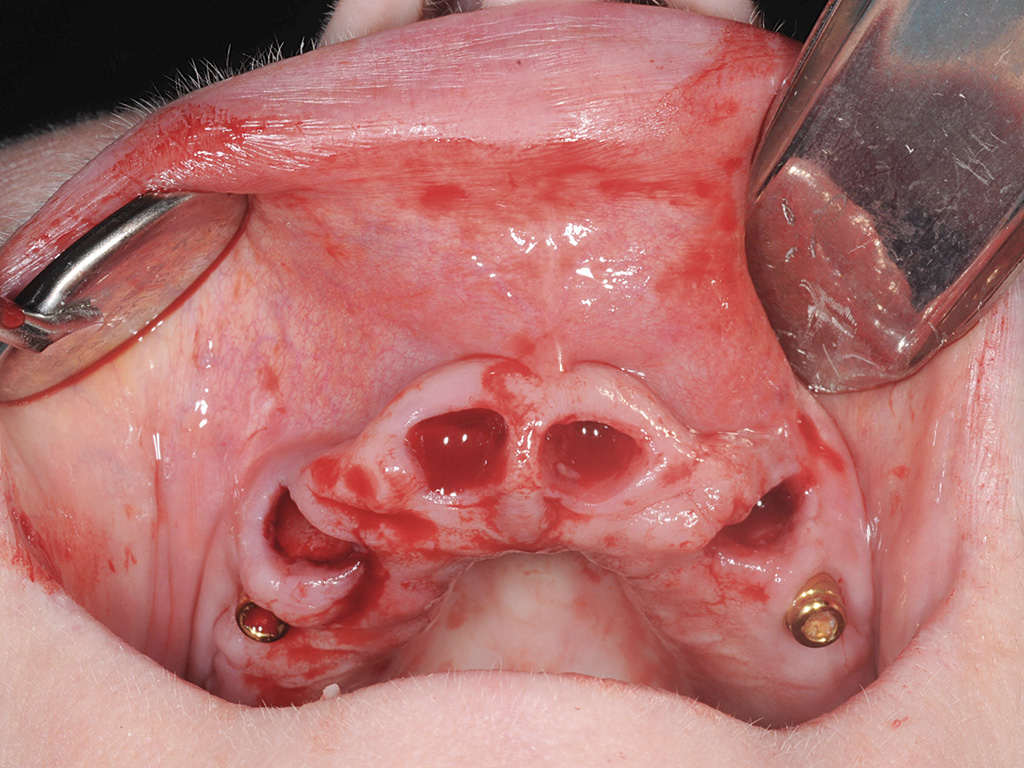
- Flange design
Restorations may incorporate deep or ridge lap flanges designed to close space, improve aesthetics and limit air and fluid escape. In these cases a pontic becomes very difficult to clean for the patient. In addition, the clinician will have no access to peri-implant tissues at maintenance visits to allow for visual inspection or to clean the area unless the superstructure is removed. If this sort of restoration is, in addition, cemented in a patient with a history of periodontitis the risk of disease developing is potentially high due to the problems it creates with oral hygiene and the difficulty of maintenance. Flange design should take into account the patient’s need to clean around the implants and beneath the pontic over the ridge and should allow for the use of interdental brushes or bridge floss in the area.
- Embrasure closure
Long and tight embrasures, designed to avoid black triangle spaces and fluid leakage, can make it extremely difficult to clean around implants when the spaces are too narrow to allow access for cleaning aids. This may be less of a problem if the patient is manually dexterous. However, if the patient is older and relying on help, for example if they are resident in a care home, the levels of oral care provided may be poor and implant health compromised.
Maintenance
Following delivery of the implant supported restoration it is essential that the patient is supported in their efforts of maintenance at home9,14,15,16. This applies whether there are remaining teeth or the dentition is implant-supported. At fitting of the prosthesis, all patients should have a good-quality periapical radiograph taken to establish baseline bone levels. If the patient has had periodontitis in the past then a comprehensive supportive care programme should be in place and can be modified to ensure adequate maintenance of the implants.
Once again plaque control was identified as a major risk for peri-implant mucosisitis in a recent systematic review17. As part of their completion review, patients should be given detailed instruction on exactly how to maintain their new restoration to avoid this. This will involve helping them to find the appropriate mechanical aids to access the peri-implant tissues and ensuring they can use them on a regular basis. At this stage, the benefits of the preparatory phase will become very apparent. Patients will already be used to and in the habit of cleaning to a high standard and have the knowledge of why that is necessary.
They may have personal experience of the benefit of periodontal treatment and support. Ideally, post-placement review should be a matter of modifying an existing good technique rather than attempting at that late juncture to introduce an entirely new one. All patients then need to understand the importance of supportive treatment either with a dentist or hygienist in ensuring long-term success of their restoration.
It is usual for patients to have an annual implant review appointment when radiographs are updated to monitor peri-implant bone levels and restorations checked. For those with retained natural teeth or with a history of periodontitis this is not likely to be adequate. A programme should be followed which will support their periodontal tissues, control inflammation and reduce risk of implant problems as well as monitoring the implants directly. For periodontitis evidence is plentiful that those following and compliant will have considerably increased chance of stability8,18.
Conclusion
In the current climate of using fixed implant-supported restorations to replace teeth, it is essential that patients are fully assessed prior to treatment. This is particularly important when considering the patient with a history of periodontitis who is at increased risk of peri-implant problems. If periodontitis is present it should be controlled prior to placement and the patient should be fully informed of their increased risk.
If periodontitis cannot be controlled then consideration should be given to a restoration not dependant on implants in a tooth/implant situation. Once placed, restorations need tight maintenance on a regular basis by both patient and dentist/hygienist. All those involved in planning and provision of implant treatment need to ensure they and their team have the skill to support their patients not only in the immediate surgical and restorative phases but in the longer-term life of the prosthesis.
About the author
Madeleine Murray, BDS, MSc, MPhil, FDS(Rest.Dent.) RCPS, MRD RCS Eng, qualified BDS from the University of Glasgow in 1984. She went on to train in the speciality of periodontics in London and then restorative dentistry in Glasgow and Manchester. Since the late 1980s, her principal clinical interest has been periodontology, especially the treatment of young individuals with aggressive periodontitis and, more recently, the management of patients with periodontitis who are having implant therapy. After specialist training, she taught on the Masters in Primary Dental Care in Glasgow and worked in specialist practice before moving with her family to Shanghai, China, for five years. She returned to Scotland in 2011 and is now based at the specialist clinic Vermilion in Edinburgh. She is an examiner for the specialist MRD in Periodontology at the Royal College of Surgeons in Edinburgh. She is married with two daughters.
References
1. Schou S1, Holmstrup P, Worthington HV, Esposito M Outcome of implant therapy in patients with previous tooth loss due to periodontitis. See comment in PubMed Commons below Clin Oral Implants Res. 2006; 17 Suppl 2: 104-23.
2. Ong CT, Ivanovski S, Needleman IG, et al. Systematic review of implant outcomes in treated periodontitis subjects. Journal of Clinical Periodontology. 2008; 35: 438-462.
3. De Boever A, Quirynen M, Courke W, Theuniers G, De Boever J. Clinical and radiographical study of implant treatment outcomes in periodontally susceptible and non-susceptible patients: a prospective long term study. Clin Oral Implants Res 2009; 20: 1341-1359
4. Mengel R, Behle M and Flores-de-Jacoby L. Osseointegrated implants in subjects treated for generalized aggressive periodontitis: 10 year results of a prospective, long term cohort study. J Periodontol 2007; 78: 2229-2237
5. Jepsen S, Berglundh T, Genco R, Aass A-M, Demirel K, Derks J, Figuero E, Giovannoli J-L, Goldstein M, Lambert F, Oritz-Vigon A, Polyzois I, Salvi G E, Schwarz F, Serino G, Tomasi C and Zitzmann N.U. Primary prevention of peri-implantitis: Managing peri-implant mucositis. Journal of Clinical Periodontology. 2015; 42(S16) S152-S157
6. Paulander J, Wennstrom JL, Axelsson P, Lindhe J. Some risk factors for periodontal bone loss in 50-year-old individuals. A 10-year cohort study. Journal of Clinical Periodontology. 2004; 31: 489-496.
7. Donos N, Laurell L and Mardas N. Hierarchical decisions on teeth vs implants in the periodontitis susceptible patient: the modern dilemma. Periodontol 2000 2012; 59: 89-110
8. Graetz C, Dörfer CE, Kahl M, Kocher T, Fawzy El-Sayed K, Wiebe JF, Gomer K, Rühling A. Retention of questionable and hopeless teeth in compliant patients treated for aggressive Periodontitis. Journal of Clinical Periodontology 2011; 38: 707-14
9. Axelsson P, Nystrom B and Lindhe J. The long term effect of a plaque control program on tooth mortality, caries and periodontal disease in adults. Results after 30 years of maintenance. Journal of Clinical Periodontology 2004; 31: 749-57
10. Suvan JE. Effectiveness of mechanical nonsurgical pocket therapy. Periodontology 2000. 2005;37:48-71.
11. Eberhard J, Jervoe-Storm PM, Needleman I, Worthington H, Jepsen S. Full-mouth treatment concepts for chronic periodontitis: a systematic review. Journal of Clinical Periodontology. 2008; 35: 591-604.
12. Cortes AR, Cortes DN, No-Cortes J, Arita ES. Transition from failing dentition to full-arch fixed implant-supported prosthesis with a staged approach using removable partial dentures: a case series. J Prosthodont. 2014; 23: 328-32
13. Piñeyro A, Ganeles J. Custom abutments alone will not eliminate the clinical effects of poor cementation techniques around dental implants. Compend Contin Educ Dent. 2014; 35: 678-80, 682-6.
14. Carnevale G, Cairo F, Tonetti MS. Long-term effects of supportive therapy in periodontal patients treated with fibre retention osseous resective surgery. I: recurrence of pockets, bleeding on probing and tooth loss. Journal of Clinical Periodontology. 2007; 34: 334-341.
15. Tonetti MS, Muller-Campanile V, Lang NP. Changes in the prevalence of residual pockets and tooth loss in treated periodontal patients during a supportive maintenance care program. Journal of Clinical Periodontology. 1998; 25: 1008-1016.
16. Zangrando MS, Damante CA, Sant’Ana AC, Rubo de Rezende ML, Greghi SL, Chambrone L. Long-term evaluation of periodontal parameters and implant outcomes in periodontally compromised patients: a systematic review. J Periodontol. 2015; 86: 201-21.
17. Renvert S and Polyzois I. Risk factors for peri-implant mucositis: a systematic literature review. Journal of Clinical Periodontology. 2015; 42(S16): S172-S186
18. Tomasi C, Wennstrom J L and Berglundh T. Longevity of teeth and implants – a systematic review. J Oral Rehabil 2008; 35(Supplement): 23-32
Verifiable CPD Questions
Verifiable CPD Questions
Aims, objectives and learning outcomes
- To discuss the assessment of patients’ periodontal status prior to implant placement
- To introduce the concept of periodontal and peri-implant risk
- To outline ways to manage risk when placing implants.
Example question
Q. What factors are important in increasing a patient’s risk of peri-implant problems?
a. Smoking
b. History of periodontitis
c. Poor oral hygiene
d. All of the above
Submit your answers listings
Comments are closed here.